The Complete Guide to Real-Time CDI for Health Systems
Most CDI programs are built around a process designed decades ago. Here is why timing is the most important variable in clinical documentation improvement, and what real-time CDI actually changes.
Clinical Documentation Integrity (CDI) has been a fixture of health system revenue cycle operations for over twenty years. And yet the standard CDI intervention, a query sent to a clinician after a chart is reviewed, still depends on a clinician answering it between clinical duties, sometimes days after the relevant encounter. The clinician answers, sometimes, and the record gets corrected. Sometimes.
This model made sense when documentation happened on paper and queries were mailed. In 2026, with AI systems capable of surfacing documentation gaps in real time, it no longer does.
This guide covers what clinical documentation improvement actually is, why the timing of intervention changes everything, how real-time CDI works in practice, and what health systems should expect when they make the shift.
1. What Is Clinical Documentation Integrity?
Clinical Documentation Integrity (CDI) is the process of ensuring clinical documentation is complete, specific, and accurate enough to support appropriate diagnosis-related group (DRG) assignment and reimbursement. Vague documentation, "anemia" instead of "iron deficiency anemia due to chronic blood loss," or "respiratory failure" instead of "acute hypoxic respiratory failure requiring mechanical ventilation", leads to lower DRG weights, lower reimbursement, and understated Case Mix Index (CMI).
The CDI function was created specifically to close this gap. Their job is to identify documentation that is clinically incomplete, query the clinician for clarification, and ensure the final record reflects the actual complexity of care delivered.
A 0.05-point increase in CMI for a 300-bed hospital typically translates to $1M or more in additional annual reimbursement. Most health systems are leaving that gap on the table every year.
2. The Problem With the Traditional CDI Query Cycle
In the standard CDI model, a specialist reviews a chart, flags a documentation gap, and sends a query to the treating clinician, who may have moved on to dozens of other patients by that point. Responding to that query is a separate task, completed outside the encounter, often hours or days later.
By the time the query arrives, clinical context has already started to fade. Industry guidelines set a 48-to-72-hour window as the standard target for response, but many programs fall short. The patient may be discharged, the details are harder to reconstruct, and the clinician is managing a full current panel. Response rates vary widely across organizations, and every unanswered query is a documentation gap that closes without resolution.
- ~70% of information is lost within 24 hours without reinforcement, meaning clinician recall degrades significantly between encounter and query
There is also a clinician experience problem. Retrospective queries arrive out of context, require mental context-switching, and feel punitive rather than supportive. Over time, this erodes the clinician-CDI relationship and reduces cooperation, the opposite of what a high-functioning CDI program needs.
3. What Real-Time CDI Actually Means
Real-time CDI surfaces documentation opportunities to the clinician at the point of documentation. Instead of a query arriving days later, the system identifies a potential gap, a missing secondary diagnosis, an insufficient complexity qualifier, a chronic condition not mentioned despite being actively managed, and presents it to the clinician while they're documenting the encounter.
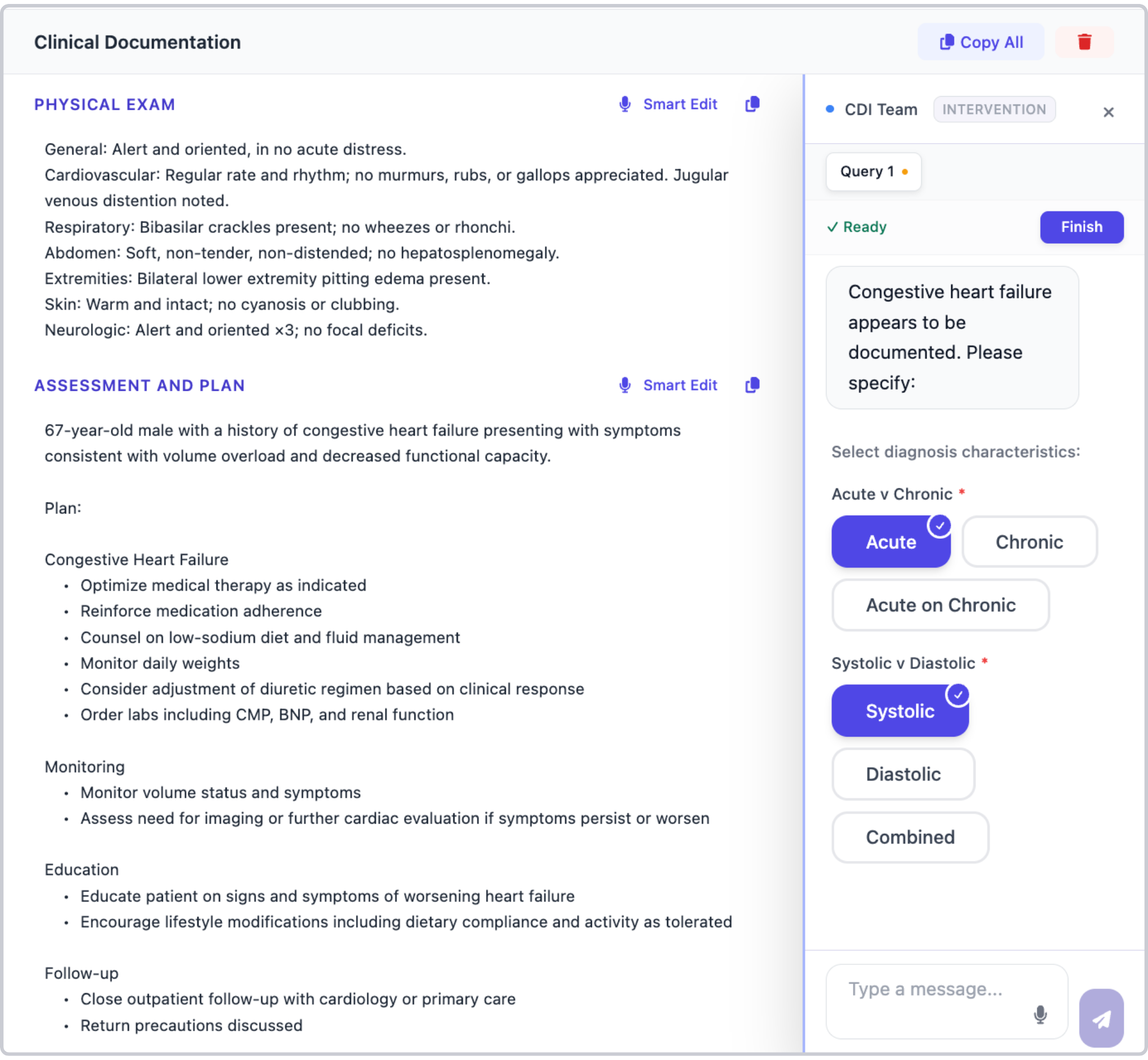
In practice, this looks like a notification in the clinician's workflow: "Congestive heart failure appears to be documented. Please specify: Acute v Chronic, Systolic v Diastolic." The clinician can specify or dismiss it in one or two clicks.
Real-time CDI is not about second-guessing clinicians, it is about surfacing the clinical complexity they are already managing so the documentation reflects the care delivered.
Why Timing Changes Everything
The fundamental advantage of real-time intervention is that it works with the clinician's clinical memory rather than against it. At the point of care, a clinician knows exactly why they managed a patient the way they did. They can confirm, clarify, or expand documentation with minimal cognitive load. Three days later, that context is largely gone.
Real-time CDI also eliminates the query-response cycle entirely for the cases it catches. There is no query to draft, no follow-up, no waiting for a clinician to respond. The documentation is completed correctly the first time, which means coding and billing can proceed without a waiting period.
4. How Real-Time CDI Integrates With Clinical Workflow
Effective real-time CDI has to live where clinicians work. Cleo surfaces CDI opportunities directly in the clinician's documentation workflow, not in a separate CDI application that requires context-switching. As a clinician completes a note, the system analyzes the clinical content against the diagnosis list, procedure documentation, and active problem set to identify specificity gaps.
Because Cleo integrates directly with the EHR and/or handles ambient documentation, the CDI layer has access to the complete clinical picture at the point of care: the live chart, the ambient note being generated from the encounter, and all relevant prior documentation. CDI opportunities are not inferred from a partial chart; they are identified against everything that is clinically known about the patient in that moment.
5. What to Expect: Metrics Real-Time CDI Moves
Health systems that implement real-time CDI typically see improvement across three categories of metrics: financial, operational, and clinical.
Financial
The most direct financial impact comes through CMI improvement. Real-time CDI consistently captures diagnoses and complexity that the traditional query cycle misses, because the clinician is available and informed at the moment of documentation. Health systems implementing AI-assisted CDI have reported CMI improvements of 5 percent or more within the first year of deployment. In Cleo's own case study data, real-time CDI contributed to an average of $243 saved per inpatient stay. The magnitude of improvement depends on baseline documentation practices and patient population complexity.
Operational
CDI specialist time shifts from high-volume retrospective query management to complex case review and program oversight. Query volume drops significantly for routine documentation specificity, the cases that real-time CDI handles automatically, freeing specialists for the cases that genuinely require clinical expertise and negotiation.
Clinical
Accurate diagnosis documentation is not just a billing issue. It affects care continuity, handoff quality, and population health analytics. When diagnoses are provided with full specificity, downstream care teams have an accurate picture of patient complexity. Real-time CDI improves the quality of the clinical record as a care coordination tool, not just as a billing artifact.
6. Implementation Considerations
Transitioning from retrospective to real-time CDI is not a rip-and-replace of your existing program. In most cases, it is a layer on top of your current workflows that gradually reduces the volume of retrospective queries your team manages.
- Existing CDI staff shift focus from routine query management to complex case review
- Clinician training is minimal, real-time prompts are designed for one-click interaction
- Program governance should be updated to track real-time vs. retrospective CDI impact separately
- CMI and DRG accuracy metrics should be baselined before deployment for comparison
The biggest implementation consideration is organizational: CDI programs that have been running retrospectively for years have processes, metrics, and workflows built around that model. Real-time CDI does not invalidate that investment, it extends it. The goal is to use real-time intervention for the cases where timing matters most and preserve retrospective capacity for complex cases that require deeper CDI expertise.
7. The Bottom Line
Retrospective CDI will always be better than no CDI. But in a healthcare environment where AI can surface documentation gaps in real time, the opportunity cost of waiting until after discharge is real and measurable. For health systems focused on CMI improvement, DRG accuracy, and reducing the administrative burden on CDI teams, real-time CDI is the highest-leverage intervention available.
Cleo's Acute Care OS integrates real-time CDI directly with ambient documentation and charge capture, so the same AI engine generating the clinical note is also surfacing CDI opportunities and coding suggestions. If you want to see what that looks like in practice, we are happy to walk through it.
Sources
- AHIMA — Clinical Documentation Integrity Key Performance Indicators Practice Brief
- ACDIS 2024 CDI Week Q&A: Query Metrics and Technology — physician query response rate benchmarks
- ACDIS — Q&A: How to Determine an Appropriate Physician Query Response Rate
- ACDIS — AI-Enabled CDI Powers 5% CMI Improvement (El Paso Children's Hospital)
- ACDIS — CDI Programs Drive Up Case Mix Index, Revenue (Heritage Valley Health System)
- Murre & Dros (2015) — Replication and Analysis of Ebbinghaus' Forgetting Curve, PLOS ONE
- AAPC — The Transition of CDI (history and evolution of CDI programs)
See Cleo in action.
Cleo unifies ambient documentation, charge capture, and real-time CDI in one platform built for acute care.
Get a Demo